Coronary bypass graft surgery (CABG) has been used for the last 25
years as an additional method of relieving angina. This it does in most cases,
usually abolishing it completely or making it much less severe. It has also
been shown to prolong life in those with advanced coronary disease. Like
all major surgical procedures, there is some risk but this is quite small.
Surgery is only recommended if angina cannot be relieved by medicines or
angioplasty or if the outlook is thought otherwise to be poor. The object of
the operation is to bypass the narrowed parts of one or more coronary
arteries by granting a blood vessel between the aorta (the main artery) and
the affected arteries beyond the parts that are blocked. Most commonly, a
piece of vein is removed from the leg for this purpose, but it is also possible
to make use of an artery that normally runs down the inside of the chest
wall. Before the decision is taken that surgery is the best option, it is
necessary to have a coronary catheterisation. This provides X-ray films of
the coronary arteries that enable the heart surgeon to see exactly where the
grafts should be placed. In order to perform the operation, the surgeon has to
open up the chest by splitting the breastbone from top to bottom, so that
afterwards there is a scar that is often likened to a zipper. Inevitably, there is
discomfort in the chest immediately after the operation but this gradually
diminishes in the succeeding days. There is also some discomfort and
swelling of the leg if a vein has been removed.
If all goes well, the patient may be sitting out of bed in a day or two
after the operation and be out of hospital in a week or so.
Patients usually return to a full life (including work) in 2-3 months.
When drugs do not provide enough relief, heart surgery may be the best
answer. For some people with particular types of narrowing of the arteries, 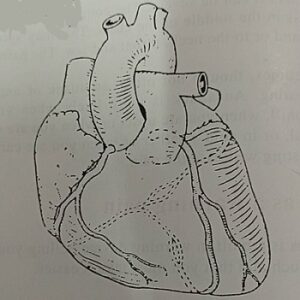 Triple coronary artery bypass graft
Triple coronary artery bypass graft
heart surgery might reduce the chances of a heart attack. A cardiologist and a
cardiac surgeon will advise on your particular case. The tests will include an
electrocardiogram (ECG) while you are exercising, and an angiogram. The
angiogram will show the exact extent of the narrowings of the arteries.
“Bypass” surgery usually takes a vein from your leg, and attaches it
alongside the narrow heart artery, but an artery may be used instead. The
vein makes a new bypass joining the heart muscle to the blood supply from
the large main artery as it leaves the heart. Angioplasty
Angioplasty
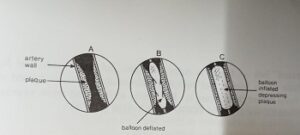
Angioplasty is a fairly new technique. It is suitable if the narrowings of
your coronary arteries are limited to fairly short lengths and are at the wider
ends of the arteries.
A fine tube, or catheter, is used. This has a balloon at its tip. The
catheter tip is moved into the narrowing, and the balloon is blown up. This
pushes back the built-up material inside the artery, so that the artery is
widened.
Angioplasty may be used, instead of surgery, for up to 25% of patients.
It needs only one to three days in hospital. If the treatment goes well then
normal life, including work, is usually possible within a week. Surgery is
always available as a back-up when angioplasty is being done.